To Your Health — and Mine
The uproar over mammogram guidelines is proof that health care reform that actually controls costs would be virtually impossible to achieve.The uproar over the on-again, off-again guidelines on when women should have mammograms is proof of the blindingly obvious: Health care reform that actually controls costs — rather than just pretending to do so — would be virtually impossible to achieve.
I say “would be” because none of the voluminous reform bills being shuttled around the Capitol on hand trucks even tries to address a central factor that sends costs spiraling out of control, which is that each of us wants the best shot at a long, healthy life that medical science can offer. Just as all politics is local, all health care is personal. Skimping on somebody else’s tests and procedures may be worth debating, but don’t mess with mine.
Intellectually, it’s simple to understand why it might make sense for women — those who have no special risk factors for breast cancer — to wait until they’re 50 to start getting mammograms instead of starting at 40. The analysis by the U.S. Preventive Services Task Force, which made the recommendation, looks sound. According to the panel, a whopping 10 percent of mammograms result in false-positive readings that lead to unjustified worry and unneeded procedures, such as biopsies. In a small number of cases, women are subjected to cancer treatment or even a mastectomy they didn’t need.
This harm, the task force reasoned, outweighs the benefits of discovering a relatively few cases of fast-growing, life-threatening breast cancer in women in their 40s through annual mammography. It is also true that waiting to begin regular mammograms until a woman reaches 50 — and reducing the frequency to once every two years, as the task force recommended — would save a portion of the more than $5 billion spent on mammography in the United States each year.
The problem lies in those relatively few instances when a mammogram does find that a woman in her 40s has a life-threatening tumor, and when early detection saves her life. This scenario may be fairly rare, but it happens. Given the option, many women would rather be safe than sorry — and safe costs money.
The analogous dilemma for men involves prostate cancer: Should men have a blood test for prostate-specific antigen (PSA), and, if so, how often? An elevated PSA level suggests, but does not prove, that prostate cancer might be present, and tells nothing about the progression of a possible tumor.
For me, “test or no test” is a no-brainer: African-American men are at elevated risk for prostate cancer, so I have had my PSA level checked at my annual physical since I was in my early 40s. So far, so good. But if the level were to spike and a tumor were to be found, I’d have to decide whether to have it treated aggressively — with radiation or surgery, both of which involve complications and risks — or undertake a period of “watchful waiting.” Many prostate cancers progress so slowly that the patient grows old and dies of something else before the tumor becomes an issue.
In other words, some men will get PSA tests year after year, then ultimately have expensive cancer treatment, to cure a disease that ultimately would not have threatened their lives. The American Cancer Society recommends that doctors discuss the pros and cons of PSA screening with their patients, but doesn’t go on to recommend that all men be screened. In March, two studies were published in The New England Journal of Medicine: One said PSA testing saves lives, the other said it doesn’t.
But PSA testing has become so routine, like mammography, that I doubt many would be willing to give it a pass. Each of us should ask ourselves this question: How much expensive, unnecessary, high-tech testing and treatment am I willing to have our out-of-control health system pay for to save one life, if the life in question might be mine or that of a loved one? The honest answer, I think, is: a whole bunch.
The honest solution is a word that cannot be spoken: rationing. Our system already rations health care based on the individual’s ability to pay. Insurance companies ration some tests and procedures based on age, risk factors and what often seems like whim. This ad hoc rationing doesn’t work very well, and nothing in any of the reform bills even tries to address the basic consensus that makes spending continue to rise: Put a lid on everybody else’s costs, but don’t touch mine.
Eugene Robinson’s e-mail address is eugenerobinson(at)washpost.com.
© 2009, Washington Post Writers Group
Your support matters…Independent journalism is under threat and overshadowed by heavily funded mainstream media.
You can help level the playing field. Become a member.
Your tax-deductible contribution keeps us digging beneath the headlines to give you thought-provoking, investigative reporting and analysis that unearths what's really happening- without compromise.
Give today to support our courageous, independent journalists.
 Global Voices
When “forever chemicals” contaminated their water, Italian mothers got organized and took the polluters to court.
Global Voices
When “forever chemicals” contaminated their water, Italian mothers got organized and took the polluters to court.
 Health & Wellness
Chevron intends to produce “climate-friendly” fuel in the Magnolia State and cancer-wary locals are concerned.
Health & Wellness
Chevron intends to produce “climate-friendly” fuel in the Magnolia State and cancer-wary locals are concerned.
 TD Original
Glyphosate is linked to the decline of honey bees and everything from cancer, autism and irritable bowel syndrome in humans.
TD Original
Glyphosate is linked to the decline of honey bees and everything from cancer, autism and irritable bowel syndrome in humans.
 Environment
Experts say the Inflation Reduction Act's push for biogas is "one step forward and two steps back."
Environment
Experts say the Inflation Reduction Act's push for biogas is "one step forward and two steps back."
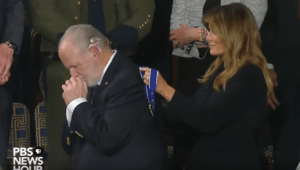 The conservative commentator, who just announced he has advanced lung cancer, is presented with the honor during Trump's State of the Union.
The conservative commentator, who just announced he has advanced lung cancer, is presented with the honor during Trump's State of the Union.
You need to be a supporter to comment.
There are currently no responses to this article.
Be the first to respond.