Is Private Equity Really ‘Taking Over’ US Healthcare?
No, it’s not. And pretending that it is obscures the real problem. Image: Adobe
Image: Adobe
If you get healthcare news from major media outlets, the industry press or even medical journals, you might conclude that private equity investors are “taking over” US healthcare. But when it comes to hospitals and doctors, you’d be wrong.
Many reporters and researchers have mistaken an episodic cycle of cynical profit-taking as a “takeover.” The reporting focuses public attention away from the power of hospital chains affiliated with universities and churches, which employ far more doctors than private equity, and the US’s refusal to exert political control of the medical industry to rein in costs and cover everyone.
One of the widely reported “abuses” by private equity–owned providers—“surprise bills” for doctors’ care delivered in hospitals— is simply the exercise of the market forces that are supposed to control costs and expand coverage, but have been failing for a half century.
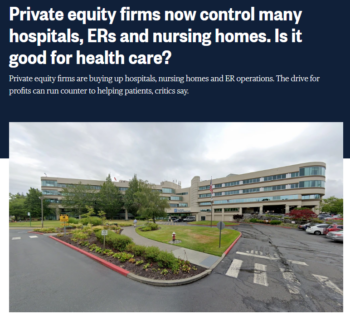
US media have been in private equity panic mode for several years now. An early entrant informed the American Prospect’s readers “How Private Equity Makes You Sicker” (10/7/19). Time (7/31/23) asked readers, “What Happens When Private Equity Buys Your Doctor’s Office?”; the New York Times (7/10/23) phrased the question as “Who Employs Your Doctor? Increasingly, It’s a Private Equity Firm.” NBC (5/13/20) reported, “Private Equity Firms Now Control Many Hospitals, ERs and Nursing Homes,” and asked, “Is It Good for Healthcare?”
KFF Health News is in the midst of a series called “Patients for Profit: How Private Equity Hijacked Healthcare.” Bloomberg (5/20/20), Common Dreams (11/29/22), Public Citizen (3/21/23), Atlantic (10/28/23), NPR (11/7/23) and a host of others have weighed in.
A bad idea
Profit-focused healthcare is a bad idea, and private equity–controlled companies have outsized influence on nursing homes and specialty hospitals, where patients are held for a long time. There is evidence that private equity–owned nursing homes kill even more patients than the rest of that chronically underfunded and understaffed industry.
But when it comes to general acute care hospitals and physician services, the degree of private equity control has been exaggerated, often with sloppy academic research. Private equity firms employ far fewer doctors than hospitals and insurance companies do, own less than 5% of general acute care hospitals, and are showing signs of exiting these segments of healthcare.
When it comes to general acute care hospitals and physician services, the degree of private equity control has been exaggerated, often with sloppy academic research.
“Private equity” is just one of many vehicles for private investment. (See “What Is ‘Private Equity,’ Anyway?”) Presenting a particular corporate structure as uniquely destructive ignores the history of boom-and-bust cycles of Wall Street investment in hospitals and doctors, and confuses readers about the ultimate winners.
The unfortunate outcome of this misunderstanding is that most media analysis promotes policy changes that apply only to private equity—like increased transparency from private equity firms, limits on some abusive real estate transactions, and post-acquisition restrictions on staffing cuts. These will do nothing to restrain extreme US healthcare costs, to expand access to healthcare or to stop actors with different corporate structures from engaging in the same abusive behavior.
Let’s do it again

The current private equity investment boom in physician practices differs little from the late 1990s, when Wall Street–backed physician practice management companies (PPMs) bought doctors’ practices by the hundreds, and then collapsed in a wave of bankruptcies. Those acquisitions were made not by private equity–controlled entities, but by companies whose stock traded openly on markets like the New York Stock Exchange and NASDAQ, known as “publicly traded” companies.
Media narratives about doctors’ experiences in the earlier Wall Street dive into medicine are nearly identical to current private equity reporting. Doctors start off hoping well-capitalized firms will bring administrative efficiency and growth, while allowing them to focus on patients. They end with unsustainable debt, bankruptcy, fraud and extreme corporate cost-cutting. Two decades apart, Fortune and Bloomberg reported identical iconic toilet paper shortfalls under lurid headlines:
As the top administrator at the 120-doctor Diagnostic Clinic in the Tampa Bay area, Robert Dippong had $250,000 in spending authority before his group became part of MedPartners in 1996. The day after the purchase, he recalls, “I couldn’t even buy toilet paper.”
—”Vulgarians at the Gate: How Ego, Greed and Envy Turned MedPartners From a Hot Stock Into a Wall Street Fiasco” (Fortune, 6/21/99)
A doctor at Advanced Dermatology says that waiting for corporate approvals means his office is routinely left without enough gauze, antiseptic solution and toilet paper.
—“How Private Equity Is Ruining American Healthcare” (Bloomberg, 5/20/20)
When the dust settled in 1999, there were two big winners in the US acute healthcare system: large tax-exempt “charitable” hospital systems, and hospital companies whose stock is sold openly on Wall Street. Not only have these players consolidated their power by acquiring smaller, financially weaker hospitals, they spent the last two decades buying up physician practices, thanks in part to the efforts of the George W. Bush and Obama administrations.
Shortly after the Wall Street–backed PPM industry imploded, the George W. Bush administration issued new Medicare payment regulations that allowed doctors employed by hospitals to charge more than traditional private practices (Federal Register, 8/1/02). Treatment in a doctor’s office is paid on a different schedule than the same treatment at a hospital’s outpatient department. The 2002 rules legally transformed doctors’ offices, miles away from a hospital’s campus, into a wing of its outpatient department. These changes allowed hospitals to add large “facility fees” on top of fees for doctors’ services, creating a big incentive for hospitals to buy doctors out.
The News and Observer (12/16/12) ran a Pulitzer-finalist series more than ten years ago describing how this process socked patients with large unexpected bills, as Duke University Medical Center and UNC Health bought up doctors across North Carolina. (More on facility fees at Healing and Stealing—10/21/23.)
Corporate consolidation of physician practices accelerated in 2009, when President Barack Obama signed a law requiring a shift to electronic medical records, which created new requirements for capital investment by physicians. Heavily endowed tax-exempt hospital chains and publicly traded hospital corporations were happy to help with those investments—in exchange for ownership or control of a practice.
Who doctors really work for
A widely reported April 2022 study—prepared by healthcare consultants Avalere for the Physicians Advocacy Institute (4/22), a nonprofit founded with money from settlements of class action lawsuits by doctors against insurance companies—found that nearly 70% of doctors are now employees, not owners of their practices.
And who employs them? Hospitals, mostly. According to the study data, 70% of doctors who are employees—52% of all US doctors—are employed by hospital systems. The remaining 30% of employed doctors—22% of all US doctors—are employed by “other corporate entities,” which “include health insurers, private equity firms, umbrella corporate entities that own multiple physician practices, etc.”
Private equity employers are only a slice of that remaining pie. Becker’s Payer Issues (2/16/23), a health insurance industry trade newsletter, reported last February that the largest employer of physicians in the US is health insurance giant UnitedHealth Group, with 70,000 “employed or aligned” physicians. Nine months later, the company disclosed that the number of “employed or affiliated” doctors had jumped to 90,000 (Becker’s Hospital Review, 11/29/23).
According to the study data, 70% of doctors who are employees—52% of all US doctors—are employed by hospital systems.
“Aligned” and “affiliated” doctors are not necessarily direct UnitedHealth employees, but insurers and major drug store chains account for a large chunk of doctors employed by “other corporate entities” (New York Times, 5/12/23).
The research on the private equity “takeover” of physician practices reveals the relatively small industrial power of those firms. A study by nonprofit and UC/Berkeley researchers warned that in 28% of US metropolitan statistical areas (MSAs), a single private equity firm had gained 30% market share in at least one of 10 specialties, and in 13%, a single firm had gained 50% market share in at least one specialty. The study was reported widely in the business press, and formed the basis for a major New York Times story (7/10/23).
Looking through the other end of the telescope, 72% of all US metropolitan areas have no meaningful private equity market power in any specialty at all. Many of the MSAs threatened by private equity are far smaller than nearby areas facing monopoly threats from university- and church-affiliated hospitals.
The Johnstown, Pennsylvania, MSA has 129,000 people. Johnstown has a PE firm with 50% market share in at least one specialty. Seventy miles away, the Pittsburgh MSA, with 2.3 million people, does not. What Pittsburgh does have is the headquarters of the tax-exempt University of Pittsburgh–affiliated UPMC health system, which generated $26 billion in revenue last year, and sits atop $23 billion in assets. UPMC has recently been the subject of antitrust scrutiny from state and federal legislators (WPXI, 1/19/23) and employs more than 5,000 doctors.
Falling off the same cliff

In a dissection of the 1990s’ PPM crash, the late Princeton economist Uwe Reinhardt (Health Affairs, 1–2/00) pointed out how the value of the PPM companies’ stock depended on a constant growth that was obviously impossible to sustain.
The companies first paid for practices with cash and stock trades. Since, beyond skimping on toilet paper, there are few “efficiencies” from owning practices in different regions, the cash soon ran out, and companies borrowed money to keep the buying spree going. That, wrote Reinhardt, “can spell disaster in periods of revenue downturns,” as the cost of paying back loans exceeds incoming profits. PPMs wound up on a fast track to bankruptcy court.
The PE investment wave has also loaded practices with debt, and is falling off the same cliff, as conditions that prompted firms to buy doctors’ practices have changed.
Decades of US policy have encouraged nearly all US health plans to use administrative rules and financial coercion to strip patients of the ability to choose their doctors and hospitals (KFF Employer Health Benefits Survey, 2023). Limiting choice to contracted physician and hospital “networks” is supposed to save money, as insurers pay providers discounted rates in exchange for higher patient volume. As cost control, it has been failing for 50 years, but as an economic opportunity for financial manipulators, it works wonders.
Emergency medicine doctors who resisted becoming hospital employees have been a prime target for PE money, taking advantage of the fact that hospitals must treat patients who show up at the emergency room (NBC, 5/13/20). If a practice that staffs a hospital’s ER doesn’t have a contract with an insurer, they bill at sticker prices much higher than the network discount. So in recent years, patients who went to network hospitals for emergencies have sometimes been treated by “out of network” emergency doctors, who bill them and their insurers at the shockingly higher rates—an appealing situation for private equity.
However, new state and federal laws have curbed surprise billing. The new laws, along with a shrinking pool of doctors who haven’t already been bought out by hospitals or insurers, have touched off a wave of debt-fueled bankruptcies and sell-offs similar to the 1990s. Even as the “takeover” drumbeat reached a crescendo, Envision Healthcare, the largest private equity–owned physician practice in the US, declared bankruptcy last May (Stat, 5/15/23). American Physician Partners, “one of the nation’s biggest employers of emergency physicians,” followed suit in July (American Prospect, 7/29/23).
The real hospital bad guys
When it comes to hospitals, Philadelphia is ground zero for misdirected media attention on private equity. In 2018, Paladin Healthcare Capital, a private equity firm controlled by investor Joel Freedman, purchased Hahnemann Hospital, promising to invest in needed improvements. Freedman instead drove the hospital into bankruptcy, after selling the land under it to another company he controlled. It’s now the site of a condo development.
Sen. Bernie Sanders (I–Vt.) made Hahnemann a symbol of his support for Medicare for All in the run-up to the 2020 primaries (CBS News Philadelphia, 7/15/19). Hahnemann became the go-to example of private equity’s aggressive takeover of hospitals with the intent of selling them to real estate developers. Eileen Applebaum, co-director of the Center for Economic and Policy Research, led with the Hahnemann story in her influential American Prospect reporting (10/7/19) on private equity, warning that
private equity firms are using borrowed money to assemble medical empires across the country. Not only do consolidated hospitals harm patients with higher prices and worse outcomes, but the shaky financial pictures that result habitually lead to massive cost-cutting and closures of unprofitable facilities, which put entire communities at risk of losing access to medical care.
But private equity has almost nothing to do with hospital industry consolidation. By the time Freedman bought and closed Hahnemann, and its St. Christopher’s Hospital for Children affiliate, they were isolated facilities, neglected by their previous owner. And they were under withering competitive pressure from tax-exempt charitable hospitals affiliated with local universities: Temple University, Thomas Jefferson University and the University of Pennsylvania.
‘More symptoms than disease’
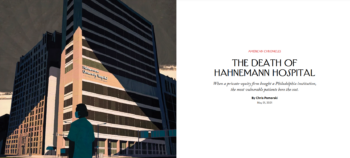
In 2021, New Yorker writer Chris Pomorski (5/31/21) published a more nuanced retrospective take on “The Death of Hahnemann Hospital.” While detailing Freedman’s managerial incompetence and the transaction that left the land under the hospitals in Freedman’s hands and out of bankruptcy as the hospital closed, Pomorski pointed out the primary villain: The hospital had been the victim of Wall Street–backed neglect for 20 years by the company that sold the hospital to Paladin—the $19 billion publicly-traded Tenet corporation.
Private equity’s maneuvers with Hahnemann, wrote Pomorski,
are more symptoms than disease. The story of Hahnemann is as much about the structural forces that have compromised many American hospitals—stingy public investment, weak regulation and a blind belief in the wisdom of the market—as it is about the motives of private equity firms.
Beyond that insight, however, Pomorski missed the bigger story in Philadelphia. As press reports noted (e.g., US News, 7/10/19), Hahnemann was a hospital that primarily treated poor patients. When it closed, patients struggled to find care at other locations, and the abrupt closure placed a heavy burden on surrounding hospitals.
Penn and Temple saw ER visits increase by 12%, and Jefferson, less than a mile from Hahnemann, by 20%, with ambulance volume doubling as emergency patients who lived close to Hahnemann dialed 911 instead of finding their own way to the emergency room. A doctor told Pomorski that the ER became so crowded, ambulances were often diverted to other hospitals, a situation known to cause unnecessary deaths. An emergency physician told Pomorski that “the ER became the scene of ‘daily human tragedies.’”
Beyond absorbing the sudden spike in patient volume and the stress it brought to frontline caregivers, at the institutional level, Jefferson and Penn played another role in Hahnemann’s woes: They were among its agents and beneficiaries.
While Tenet was neglecting Hahnemann, wealthy university hospitals were building medical empires, with “satellite hospitals, physician practices and urgent-care centers.” Pomorski quotes a Hahnemann executive criticizing Freedman for failing to negotiate higher insurance rates to stave off bankruptcy.
Telling details
The details are telling. Hahnemann’s competitors, like other large tax-exempt systems, flex their market power to drive up prices. They commanded prices so much higher than Hahnemann that the executive thought it might cost insurers less to give Hahnemann a small raise than to shift its patients to the charitable competitors.
After interviewing two patients who struggled to find specialist doctors when Hahnemann closed, Pomorski also interviewed Jefferson CEO Bruce Meyer. Jefferson hired eight Hahnemann-affiliated ob-gyn doctors to care for Hahnemann patients, but Pomorski neglected to ask why Jefferson didn’t simply hire the rest of Hahnemann’s specialists immediately and absorb their patients. After all, Jefferson had the money to start building a new $762 million specialist physician office tower three-fourths of a mile from the Hahnemann site, months before the New Yorker piece ran (WHYY, 9/10/20).
Hahnemann’s competitors, like other large tax-exempt systems, flex their market power to drive up prices.
Penn was in an even stronger position to deal with the challenges. When Hahnemann closed, Penn was already building a palatial new $1.6 billion, 504-room hospital across the street from the existing Hospital of the University of Pennsylvania (Philadelphia Inquirer, 10/30/21). The “Pavilion” opened just four months after the New Yorker piece, and includes a new two-story state-of-the-art emergency department, with 61 private rooms (Penn, 10/21/21).
Some problems in nearby ERs were likely inevitable, given that Freedman closed Hahnemann suddenly. But sitting two miles from Hahnemann with a $21 billion endowment, Penn had the resources necessary to figure out how to transition Hahnemann’s patient volume to new locations. The ultimate outcome of Hahnemann’s demise for Penn, Jefferson and Temple is a market with one less competitor, one less hospital willing to take lower rates from insurers.
The real hospital story in Philadelphia is that major nonprofit health systems are at the tail end of a 15-year, $9 billion building boom. The Pavilion is reportedly the largest capital project in Penn’s history (Philadelphia Inquirer, 10/30/21), but soon won’t even be the priciest hospital in its own neighborhood. The closely allied Children’s Hospital of Pennsylvania (CHOP), which shares a campus with Penn’s hospital, is building its own $1.9 billion new tower (Philadelphia Inquirer, 3/1/20). CHOP says they won’t need to borrow money for the project, but will pay with cash on hand, profits and contributions.
As this article was going to press, Jefferson Health announced a proposed merger with Lehigh Valley Health System. If approved, the merger would create a 30-hospital system across eastern Pennsylvania. The new Jefferson system would become Pennsylvania’s largest employer, surpassing the current champion—the University of Pennsylvania. The combined systems generated $13.8 billion in revenue last year (WHYY, 12/19/23). The question is whether all those billions in construction and revenue will afford Hahnemann’s low-income patients better or even the same treatment as they found at Hahnemann.
Who’s taking over whom?

The idea that Hahnemann could become a pattern has been a critical element in the private equity takeover, or “hijacking,” narrative. According to CNN (7/29/19), “advocates worry other private equity firms may try it with struggling hospitals in gentrifying neighborhoods all over the US.” In reality, Hahnemann is an example of grotesque wealth extraction from a dying hospital bludgeoned by neglect from a publicly traded company and competition from massively endowed urban “nonprofit” hospitals. Private equity won’t be “taking over” those winners any time soon.
In Connecticut, the reverse is happening. In 2015 and 2016, private equity firm Prospect Medical Holdings bought three tax-exempt hospitals and converted them to for-profit status (CT Mirror, 5/25/16). Prospect bought the financially struggling hospitals after the collapse of a bid from a short-lived partnership between publicly traded Tenet and Yale-New Haven Health, the state’s largest tax-exempt chain, because Tenet found state regulators’ proposed conditions to protect the public “too burdensome” (CT Mirror, 5/31/15).
Prospect’s purchase and conversion was supposed to inject capital into financially struggling Waterbury, Manchester and Rockville hospitals. Eight years later, Prospect is selling all three hospitals. The buyer? Yale-New Haven Health.
The deal gives Yale-New Haven an anchor in Waterbury, Connecticut’s fifth-largest city, where the only other hospital is owned by Trinity Health, a nationwide tax-exempt Catholic chain with 101 hospitals (and a “family” of “nearly 36,500 physicians”). As is common, Prospect moved the real estate to a different subsidiary and leased the land back to its hospital entity, a maneuver documented in detailed local reporting (CT Mirror, 11/16/23).
Yale-New Haven wants state subsidies to deal with the hospitals’ financial distress, even though the YNH system had more than $4 billion in net assets at the end of the 2022 fiscal year, and drives patients to its facilities in close partnership with Yale University, which runs the state’s largest physician specialty practice and has a $41 billion endowment.
Blaming vultures for the kill
Beyond Hahnemann, rural hospitals are a major focus of private equity media coverage. Some long form reporting on rural hospitals acknowledges the transient nature of private equity investment, but coverage still tends to blame vultures who are actually feeding on carcasses killed by others.
Rural hospitals have been in systemic crisis for decades. A 2022 report (Bipartisan Policy Project, 5/22) estimated that more than 20% are at risk of service reductions or closure. Before closure, desperate owners often cut staff and shut down services, requiring some patients travel long distances for certain types of care. As with Hahnemann, private equity firms have taken advantage of the crisis in some areas, buying hospitals and stripping assets, but the death throes most often are brought on by other owners and failed policy.
In a 3,000 word story headlined “Buy and Bust: When Private Equity Comes for Rural Hospitals,” KFF Health News (6/15/22) described how Noble Health, a three-year old PE firm bought and closed Audrain Community Hospital and Callaway Community Hospital in rural Missouri. Reporter Sarah Jane Tribble makes the anguish and anger of caregivers and patients palpable, but, as with Hahnemann, Audrain was on life support when Noble pulled the plug:
Audrain had struggled before Noble came calling, said Dr. Joe Corrado, a longtime surgeon at the hospital: On an average day in 2019, 40% of beds were empty, as more treatments moved to the outpatient setting and some patients drove an hour to larger hospitals for specialty care.

Distorted research fuels panic
Distorted academic research has fueled the past four years of private equity media panic. The KFF Health News piece on rural hospitals cited a 2021 Health Affairs study (5/21) showing that private equity investments in hospitals “increased 20-fold from 2000 to 2018, and have only accelerated since.” But the study doesn’t credibly support the idea that private equity is “taking over” hospital care at all.
The researchers found “a total of 42 private equity acquisitions involving 282 unique hospitals occurred during the period 2003–17,” which means it took private equity 15 years to make deals involving 5% of US hospitals. The vast majority of these hospitals were owned by private equity for a short period of time, and 74% of the deals involved hospitals that were already for-profit, many bought from companies with their own track records of fraud and national reports of patient abuse.
More than half of the hospitals were bought in just one 17-year-old deal that bears little resemblance to the stories common in major media today. In 2006, Bain Capital bought HCA, the largest for-profit hospital company in the US (CNN, 7/20/06). It was the third time the company “went private.” Six years later, HCA started selling stock publicly again, giving a windfall to Bain and the family of former Senate Majority Leader Bill Frist, whose father founded the company (New York Times, 8/14/12).
Before the Bain deal, when the company was known as Columbia/HCA and its stock traded publicly, the hospital chain coughed up what was then the biggest Medicare fraud settlement in history, and faced national publicity about quality of care concerns (Department of Justice, 6/26/03; Vanity Fair, 8/1/98).**
In reality, hospital ownership patterns have been relatively stable since 2000, except that public hospitals are slowly disappearing. According to KFF reporting of American Hospital Association data (2000, 2021), at the turn of the century 61% of community hospitals were private not-for-profits, 15% were for-profit and 24% public. In 2021, 58% of the nation’s community hospitals remained nonprofit, and 24% were for-profit, with much of their growth at the expense of public facilities, whose share dropped to 18%.
In reality, hospital ownership patterns have been relatively stable since 2000, except that public hospitals are slowly disappearing.
Data downloaded from the nonprofit Private Equity Stakeholder Project shows that just 390 hospitals are owned by private equity firms, or less than 7% of all hospitals (PE Hospital Tracker, accessed 12/12/23). The majority are psychiatric, long-term acute care and rehabilitation hospitals, specialty facilities whose reimbursement patterns are attractive to private equity investors. Less than 4% of general acute care hospitals are owned by private equity firms.
The Hospital Tracker has useful data (it’s maintained by former colleagues of mine), but the PE Stakeholder Project’s research isn’t immune from pumping numbers up with “takeover” hot air. The web page for the tracker says “34% of private equity hospitals serve rural areas,” a claim repeated by Stakeholder Project researchers in a Health Affairs article (12/18/23) headlined “Private Equity: The Metastasizing Disease Threatening Healthcare.” Thirty-four percent sounds like a big number, but 34% of less than 7% isn’t much. According to the tracker’s data, less than 5% of all rural hospitals are owned by private equity firms.
Bad behavior all around
While some media have fed the public a litany of private equity horror stories, other journalists continue to report that “Nonprofit Hospitals Are Big Business,” as the title of a 2022 Wall Street Journal series (7/25/22–12/26/22) puts it. The Journal and others, including outlets simultaneously reporting on the private equity “takeover,” have demonstrated that tax-exempt and publicly traded hospitals yield to no one in their commitment to wealth extraction and harmful operations, including:
Staff cuts: Private equity coverage often focuses on hospital cost-cutting. At the same time, systematic staffing reductions by Ascension Health prompted an in-depth New York Times investigation (12/15/22) that found that the 140-hospital Catholic system “spent years reducing its staffing levels in an effort to improve profitability, even though the chain is a nonprofit organization with nearly $18 billion of cash reserves.”
Price increases: KFF Health News and others have reported that insurance payments to gastroenterologists, ophthalmologists and dermatologists in private equity practices are higher than those in non–private equity practices, based on a 2022 study by Johns Hopkins and Harvard researchers (JAMA Network, 9/2/22). The study found that payments to PE-owned practices were 11% higher than a control group.
The Journal and others, including outlets simultaneously reporting on the private equity “takeover,” have demonstrated that tax-exempt and publicly traded hospitals yield to no one in their commitment to wealth extraction and harmful operations.
However, the researchers only compared the prices to doctors in the shrinking universe of independent practices, excluding those “with other corporate ownership and hospital or health system affiliation” from the control group.While the independent doctors had lower prices, including hospital-owned practices may have yielded a different result. A 2018 Journal of Health Economics study (4/22/18) found that “the prices for the services provided by [hospital] acquired physicians increase by an average of 14.1% post-acquisition,” and by more “when the acquiring hospital has a larger share of its inpatient market.”
Closure of Services: Eliminating unprofitable services is a constant theme of reporting on private equity–owned hospitals, especially in rural areas. According to the Wall Street Journal (4/11/21), after then–publicly traded Lifepoint merged two hospitals in Riverton and Lander, Wyoming and rebranded them SageWest, the company closed Riverton’s ob/gyn unit, forcing patients to travel the 30 miles to Lander to deliver babies. Under community pressure, Lifepoint announced that they’d reopen the services, but the company reversed itself again after being bought by the private equity firm Apollo.
These closures and consolidations are endemic to the crisis-wracked rural hospital landscape, regardless of ownership. In Connecticut, rural residents waged an identical three-year community struggle to maintain ob/gyn services after tax-exempt Hartford HealthCare bought Windham Hospital. The conflict received both local and national coverage (US News/NBC, 11/21/21). The state finally approved the closure this month, so patients will have to make the 17-mile trek to the nearest ob/gyn unit. Now the tax-exempt owners of two of the state’s three other rural hospitals, Nuvance Health and Catholic Church-affiliated Trinity Health, have also applied to close their ob/gyn services (CT Mirror, 12/11/23).
Wrong focus yields useless policies
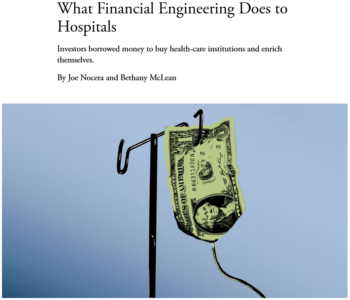
Media healthcare misdirection matters because it fuels useless policy solutions, most evident in the conclusions of long form articles in leading opinion magazines and health research journals. After regaling readers with shocking stories and sometimes misleading data, the articles typically wind up pointing to a suite of policies like those found in the recent Health Affairs article (12/18/23) from Private Equity Stakeholder Project staffers Emily Stewart and Jim Baker, and a piece by Joseph Nocera and Bethany McLean in the Atlantic (10/28/23): increased transparency, making it easier to sue private equity owners, and restrictions on financial manipulations like real estate sale-leaseback arrangements.
To their credit, Nocera and McLean inform their readers that private equity firms “appear to have lost interest in acquiring more” hospitals, but the story’s conclusion focused only on solutions to this admittedly vanishing problem, in particular Sen. Elizabeth Warren’s Stop Wall Street Looting Act.
Some of these proposals are sound general public policy, and banning private equity from nursing homes altogether probably makes sense. But a set of proposals targeting one specific corporate structure that controls relatively small slices of physician and hospital services for financial regulation has no chance to meaningfully improve a healthcare system that sends thousands of people to unnecessary deaths, and millions into debt and bankruptcy each year. These policies are a get-out-of-jail-free card for politicians on healthcare policy, allowing them to hold shocking hearings without actually fixing the country’s mess.
Until public officials decide to treat healthcare as a public good, the cycles of exploitation and patient harm will continue, regardless of the corporate structure of hospitals and physician practices. The Atlantic chose to highlight Warren’s bill as potential policy, but could have pointed in a different direction. Warren’s original cosponsors include House Progressive Caucus Chair Pramila Jayapal (D-Wash.), lead sponsor of the House version of the Medicare for All Act.
The residents of Riverton, Wyoming, have recognized the need for public investment in rural healthcare. They’ve formed a medical district to raise money for a new, publicly controlled hospital. After five years of organizing and planning, the community broke ground in July (Riverton Ranger, 7/15/23).
The community’s work is inspiring, but it also closes a circle that indicts generations of political leaders across the US for failing to accept responsibility for our healthcare system. Decades before private equity giant Apollo bought LifePoint, and years before Riverton’s Hospital was included in a group of rural hospitals that Columbia/HCA spun off to form publicly traded LifePoint, what is now called SageWest Riverton Hospital was a public hospital, controlled by the local community.
*In 2014 and 2015, I lobbied for UNITE HERE! on parts of two bills that dealt with these issues.
**I worked with SEIU on a campaign to organize Columbia/HCA workers in Las Vegas from 1997–99.
Your support matters…Independent journalism is under threat and overshadowed by heavily funded mainstream media.
You can help level the playing field. Become a member.
Your tax-deductible contribution keeps us digging beneath the headlines to give you thought-provoking, investigative reporting and analysis that unearths what's really happening- without compromise.
Give today to support our courageous, independent journalists.
 TD Original
For the chronically ill and people with disabilities, life on the streets and in shelters presents a unique set of challenges.
TD Original
For the chronically ill and people with disabilities, life on the streets and in shelters presents a unique set of challenges.
 With Joe Biden’s primary victory imminent, the 2020 election increasingly looks like a battle not for America's future but for its past.
With Joe Biden’s primary victory imminent, the 2020 election increasingly looks like a battle not for America's future but for its past.
 The Minnesota senator, best known for her questioning of Supreme Court Justice Brett Kavanaugh in 2018, says she is endorsing Joe Biden.
The Minnesota senator, best known for her questioning of Supreme Court Justice Brett Kavanaugh in 2018, says she is endorsing Joe Biden.
 Its decision on an appeal of a lower-court ruling declaring part of the statute unconstitutional is unlikely to come before the election.
Its decision on an appeal of a lower-court ruling declaring part of the statute unconstitutional is unlikely to come before the election.
 Maurice Mitchell of the Working Families Party and activist Jennifer Epps-Addison urge the left to focus on defeating corporate Democrats.
Maurice Mitchell of the Working Families Party and activist Jennifer Epps-Addison urge the left to focus on defeating corporate Democrats.
 As bad as things may look, as despairing as we can feel, it's important to remember that our country's greatest strength is its resilience.
As bad as things may look, as despairing as we can feel, it's important to remember that our country's greatest strength is its resilience.
The solution to the lack of affordable healthcare is government funded healthcare paid out of the country's tax revenue base. Call it Universal Healthcare or Single Payer Healthcare or whatever. And if the cost to do so seems too daunting the government has the power to raise the tax rates on Wealth in all its forms to increase the total revenue base.